Improving Access to Care for Children with Cardiac Disease Across Queensland
By Dr Ben Auld, AusHSI PhD Scholar
My PhD studies have been an unexpected extension of some work being done at the Queensland Children’s Hospital (QCH) to improve care to our heart kids.
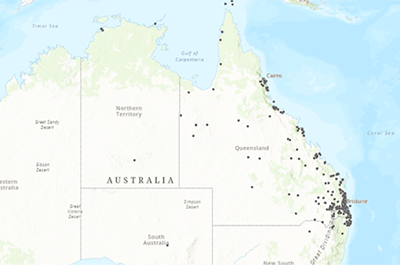
To give you some context, up to 25% of infants with congenital heart disease have critical lesions that require intervention within four weeks of birth to survive. That roughly equates to two in every one thousand births. Many more than this need intervention within the first twelve months of life and these ‘at-risk’ patients require close clinical follow up and care to avoid life-threatening changes in their heart condition. In Queensland, providing this care has a significant geographical context. Our state is three times the size of Texas with one sixth of the number of tertiary cardiac centres for children. Many patients live a long way from the only tertiary-level hospital (QCH) in Brisbane. This map (pictured) shows where our ‘at-risk’ patients have lived over the last three years. It was created with a little bit of help from geographical mapping software and some kind staff at QUT!
As one of the paediatric cardiologists working at QCH and regionally at the Gold Coast University Hospital I am part of a small team looking at neurodevelopmental outcomes for our children with heart disease. From this came an opportunity to collaborate with AusHSI on a large MRFF grant which we are currently working hard on for the CHD LIFE+ project. This grant enables us to evaluate a clinical care pathway which was created to monitor the development of children post cardiac surgery. Through further collaboration with AusHSI I embarked on a PhD looking at overall access to care for our paediatric cardiac patients across the state and empowering primary care providers to help address the problem of patients’ distance to the cardiac care unit in Brisbane. This also lines up with a new initiative in the cardiac unit at QCH to establish a clinical care network for our cardiac patients across the state.
What we hope to do with these efforts is to not only make service-level changes across the state to give our geographically remote patients a more equal share of cardiac care, but also to work out what changes will truly work. The opportunity to work with AusHSI has been fundamental to this. As clinicians we have some ideas on what good care involves, however bridging the gap between an idea and meaningful change has been the preserve of the AusHSI team. And while the work definitely keeps you busy, it has made all the difference to squirrel away on a task knowing that it is likely to be worthwhile.



